
مقدمة
That sharp or dull ache in the front of your chest during bench press can turn a rewarding workout into a frustrating experience. Pectoralis major tendonitis ranks among the most common overuse injuries in weightlifting, yet many lifters dismiss it as simple muscle soreness until it starts interfering with their training. This condition develops when the powerful tendon that attaches your chest muscle to your upper arm bone becomes irritated from repetitive heavy loading, particularly during pressing movements. While complete rest may help in the short term, stubborn cases often require more targeted support. This article explores what pectoralis major tendonitis looks like in weightlifters, how shockwave therapy may support tendon healing, and what you can do to manage this condition without giving up your fitness goals.
1. Understanding the Pectoralis Major Tendon in Weightlifting
The pectoralis major is the large chest muscle responsible for pushing movements. Its tendon connects this muscle to the humerus, the upper arm bone. In weightlifting, this structure endures tremendous force with every repetition.
1.1 What Makes the Pectoralis Major Tendon Vulnerable
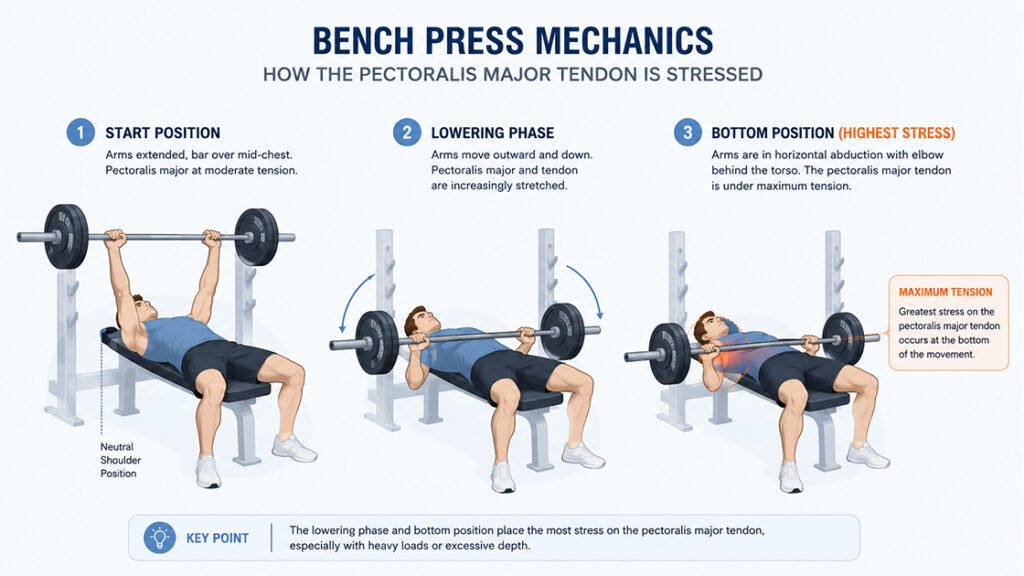
The pectoralis major is an exceptionally powerful muscle, capable of generating high forces during bench press, dips, and flyes. The tendon attaching this muscle to bone receives concentrated mechanical stress, especially during the lowering (eccentric) phase of a lift. As the arm moves outward and the elbow travels back behind the body under heavy weight, the tendon reaches near-maximal tension. With each heavy set, microscopic stress accumulates within the tendon tissue. When this stress exceeds the tendon‘s natural repair capacity, inflammation and degenerative changes begin to develop.
1.2 How Bench Press Mechanics Contribute to Tendon Strain
The bench press position places the pectoralis major tendon under a unique stress profile. When you lower the barbell to your chest, your arms move into horizontal abduction, stretching the pectoralis muscle and tendon significantly. The most common mechanism of injury occurs during this lowering phase, particularly when using heavy loads or when the chest muscles are already fatigued from prior sets. Lifters who bring the bar down too low on the chest or who use excessively wide grip positions may place even greater strain on the tendon’s insertion point near the shoulder.
1.3 Recognizing the Signs of Pectoralis Major Tendonitis
Pectoralis major tendonitis typically presents as a dull, aching pain in the front of the shoulder or upper chest. Many lifters first notice it during bench press, especially at the bottom of the movement or during the initial push off the chest. The discomfort often worsens with continued lifting and may persist after training. Some individuals experience tenderness when pressing on the tendon near the armpit area. Unlike muscle soreness that resolves within a day or two, tendonitis-related discomfort tends to linger and may gradually increase in intensity over subsequent workouts if left unaddressed.
2. What Happens Inside the Tendon
Tendonitis is not simply inflammation. The underlying pathology of chronic overuse tendon conditions involves degenerative changes within the tendon matrix that require specific management approaches.
2.1 From Acute Irritation to Chronic Degeneration
When a tendon experiences repetitive overload beyond its capacity, the collagen fibers that make up the tendon begin to disorganize. Under normal conditions, collagen fibers align neatly to provide strength and elasticity. With sustained overuse, this orderly arrangement breaks down, and the tendon develops areas of degeneration without significant inflammatory cells. This explains why traditional anti-inflammatory medications often provide limited benefit for chronic tendon issues. The problem is not primarily inflammation but structural change within the tendon tissue itself.
2.2 Why Rest Alone Often Falls Short
Taking time off from pressing movements may temporarily reduce symptoms, but the underlying tendon changes often persist. When a lifter returns to heavy training, the same mechanical stresses that caused the problem in the first place tend to bring the discomfort back. The tendon has not had the opportunity to remodel and strengthen. This cycle of rest, return, and reinjury can frustrate even the most disciplined athletes. More targeted approaches that actively stimulate the tendon‘s healing response may offer better long-term outcomes than passive rest alone.
3. How Shockwave Therapy Supports Tendon Healing
Shockwave therapy, also known as extracorporeal shockwave therapy (ESWT), delivers acoustic pressure waves to injured soft tissues. This non-invasive approach has gained recognition for its ability to support healing in chronic tendon conditions.
3.1 The Biological Mechanism: Mechanotransduction
When shockwaves pass through the skin and reach the affected tendon, they create a phenomenon called mechanotransduction. The acoustic energy converts into biological signals within the tendon cells. This mechanical stimulation triggers the body’s natural repair mechanisms, including increased blood flow to the treated area and activation of tendon-building cells called tenocytes. Over a series of treatments, these cellular responses may help remodel disorganized collagen fibers into a stronger, more functional tendon structure.
3.2 What a Shockwave Session Looks Like
A typical shockwave therapy session focuses on the painful area of the tendon. The practitioner applies a coupling gel to the skin and then uses a handheld device to deliver acoustic pulses directly to the affected site. Most patients describe the sensation as somewhat uncomfortable but tolerable, with the intensity adjustable to remain within the individual‘s comfort level. Each session generally lasts between four and five minutes. Multiple sessions, often spaced several days apart, are typically recommended to achieve optimal results.
3.3 Evidence for Shockwave in Tendinopathy
Research has demonstrated the effectiveness of shockwave therapy for various tendinopathies, including rotator cuff tendinopathy, patellar tendinopathy, and Achilles tendinopathy. While direct studies on pectoralis major tendonitis are less common, the underlying mechanism of mechanotransduction applies across different tendon locations. Shockwave therapy has shown particular promise for chronic tendon conditions that have not responded adequately to conventional conservative care. This makes it a reasonable option for lifters who have tried rest and rehabilitation without achieving lasting relief.
4. Practical Management Strategies for Lifters
Managing pectoralis major tendonitis requires more than any single intervention. A thoughtful combination of activity modification, technique refinement, and supportive therapy tends to produce the best outcomes.
4.1 Identifying and Modifying Aggravating Factors
The first step in managing this condition involves identifying which specific movements trigger your symptoms. For many lifters, the flat barbell bench press is the primary offender, particularly when using a wide grip or lowering the bar too low on the chest. Switching to dumbbell presses, which allow a more natural range of motion and grip rotation, may reduce tendon strain. Some lifters find that an incline bench press position takes pressure off the tendon while still allowing productive chest training. Reducing training volume and frequency for pressing movements can also give the tendon the recovery window it needs.
4.2 The Role of Proper Technique
Small adjustments to your bench press form can significantly reduce stress on the pectoralis major tendon. Keeping your elbows at about a 45-degree angle to your torso, rather than flaring them out wide, maintains better shoulder mechanics. Lowering the bar to the lower part of your chest rather than your upper chest also decreases strain at the tendon insertion. Avoiding the bounce at the bottom of the movement and controlling the descent helps prevent the sudden tensile loads that can aggravate an already irritated tendon.
4.3 Complementary Approaches
Several supportive measures can be used alongside shockwave therapy. Applying cold to the affected area after training may help manage post-workout sensations. Gradual eccentric strengthening, meaning exercises that focus on the lowering phase of a movement, can help remodel tendon tissue when performed appropriately. Working with a physical therapist who understands weightlifting mechanics provides personalized guidance for returning to heavy training safely.
5. Returning to the Bench Safely
Rehabilitating pectoralis major tendonitis requires patience, but most lifters can return to their previous training levels with the right approach.
5.1 Starting Light and Building Slowly
Returning to bench pressing too quickly often leads to relapse. Begin with light weights that do not provoke symptoms, focusing on controlled technique. Gradually increase the load over several weeks, monitoring how the tendon responds after each session. A small amount of discomfort during the movement may be acceptable as long as it settles within a few hours and does not worsen from session to session. If pain persists or intensifies, reducing the load further or taking additional rest days may be necessary.
5.2 Listening to Your Body‘s Signals
Tendon discomfort serves as important feedback about loading tolerance. Sharp or worsening pain during a lift signals that the tendon is not ready for that load. Dull achiness that resolves by the next day may be an acceptable part of the rebuilding process. Keeping a simple training log that notes how the tendon feels before, during, and after each session helps track progress and guides decision-making about when to advance or back off.
5.3 When to Seek Professional Guidance
If discomfort persists despite several weeks of modified training, or if you experience sudden, sharp pain with bruising around the chest or armpit, consult a healthcare provider. Complete tendon tears, though less common, require prompt evaluation. A sports medicine physician or physical therapist familiar with weightlifting injuries can confirm the diagnosis and design a specific treatment plan. They can also determine whether shockwave therapy would be an appropriate option for your particular situation.
الأسئلة الشائعة
Q1: How can I tell if my chest pain is tendonitis or a muscle tear?
Tendonitis typically develops gradually with dull aching during pressing movements. A tear often causes sudden, sharp pain with bruising and noticeable weakness. See a provider if you suspect a tear.
Q2: Can I still train other muscle groups with pectoralis major tendonitis?
Yes. Lower body exercises and pulling movements that do not stress the chest tendon are generally safe. Avoid any movement that reproduces the discomfort.
Q3: How many shockwave therapy sessions are typically needed for tendonitis?
Many protocols involve three to six sessions spaced several days apart. Your practitioner will recommend a schedule based on your response to treatment.
السؤال 4: هل العلاج بالموجات الصدمية مؤلم؟
Most people describe the sensation as uncomfortable but tolerable. The intensity can be adjusted to remain within your comfort level.
Q5: Does shockwave therapy work for all types of tendonitis?
Research supports its use for many chronic tendinopathies. However, individual responses vary. A healthcare provider can determine whether it is appropriate for your condition.
Q6: When can I return to heavy bench pressing after treatment?
Returning to heavy weights requires patience. Start with light loads and gradually increase over weeks. The tendon needs time to remodel and strengthen.
الخاتمة
Pectoralis major tendonitis can disrupt any weightlifter‘s training momentum, but understanding the condition opens the door to effective management. The repetitive heavy loading inherent to bench pressing and similar movements places genuine demands on this tendon, and when recovery cannot keep pace with training stress, discomfort follows. Shockwave therapy offers a non-invasive approach that may support the tendon’s natural healing processes through mechanotransduction, potentially helping lifters manage chronic symptoms without abandoning their fitness goals. It does not bypass the need for proper technique, gradual loading, and adequate recovery, but it may serve as a valuable supportive tool when used appropriately. By combining smart training modifications, attentive body awareness, and supportive therapies like shockwave therapy, weightlifters can address pectoralis major tendonitis and continue progressing safely.
المراجع
Shockwave Therapy – What is it and how can it help me? Vitalis Physiotherapy.
https://vitalisphysiotherapy.com.au/shockwave-therapy
Pectoralis Major Tendon Tears. OrthoPedia Patient.
https://patient.orthopedia.com/pectoralis-major-tendon-tears
Investigating the effectiveness of extracorporeal shockwave therapy at reducing pain in patients with chronic patellar tendinopathy when compared to exercise. (2024). University of Malta.
https://www.um.edu.mt/library/oar/handle/123456789/131139
How Shockwave Therapy Works. ShockwaveMachines.com.
https://www.shockwavemachines.com/how-shockwave-therapy-works
Shockwave Therapy for Musculoskeletal Conditions. Beacon Orthopaedics & Sports Medicine.
https://www.beaconortho.com/alternative-treatments-for-musculoskeletal-pain