
مقدمة
The alarm clock rings. You swing your legs out of bed, place your foot on the floor, and a sharp, stabbing pain shoots through your heel. It feels like stepping on a nail buried deep under the skin. Every morning starts this way. After a few limping steps, the pain eases, but the damage to your morning mood is already done. For millions of women who wear high heels to work and spend long hours standing on their feet, this morning ritual is a daily reminder that heel pain is slowly taking over their lives. Heat‑activated patches, over‑the‑counter painkillers, and gel heel cups offer temporary relief, but the pain keeps returning. Extracorporeal shock wave therapy (ESWT) offers a completely different approach. Instead of temporarily numbing the symptoms, it uses acoustic waves to help the body heal the plantar fascia from within. This article compares daily patch and pill use with shockwave therapy — and examines which method truly helps you take those first morning steps without dread.
1. How Heel Pain Develops and Why It Feels Like Knives on the First Step
Heel pain that strikes hardest with the first steps of the day has a distinctive name in medical literature: post‑static dyskinesia. It is the hallmark of plantar fasciitis, often accompanied by a bony heel spur visible on X‑ray. Understanding why this happens — and why it keeps returning — is the first step toward choosing the right treatment path for the long term.
1.1 What Is Plantar Fasciitis and How Does a Heel Spur Develop?
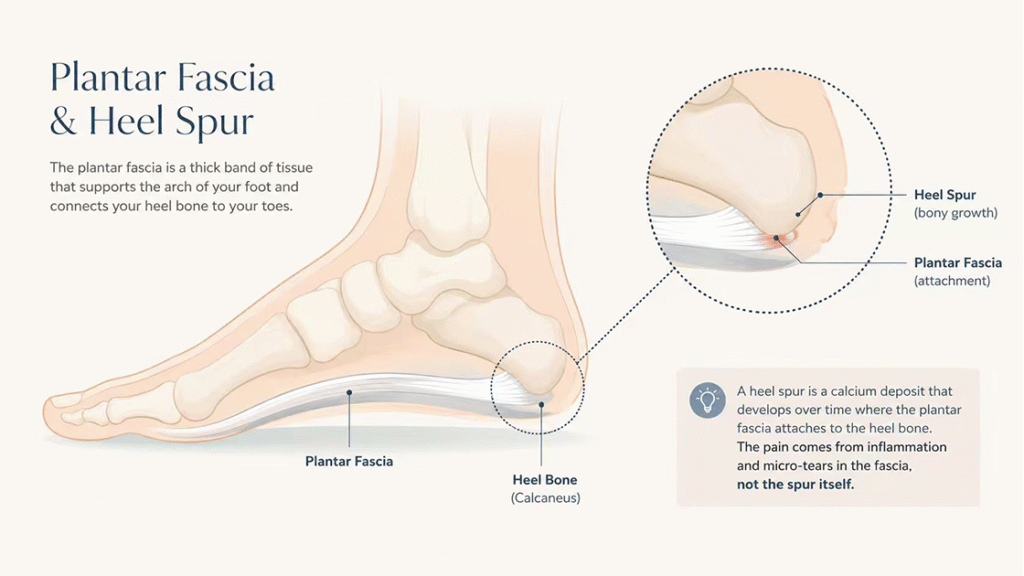
The plantar fascia is a thick band of tissue that runs along the bottom of the foot, supporting the arch and absorbing shock during walking. When this tissue is placed under chronic excessive tension — often due to wearing unsupportive footwear, spending long hours standing on hard floors, or having tight calf muscles — micro‑tears develop at its attachment point on the heel bone. Over time and with continued stress, the muscle pulls at its attachment and eventually produces a calcified spur visible on X‑ray. Contrary to popular belief, the spur itself is not the primary cause of the sharp morning pain; rather, the real source of discomfort is the surrounding inflammation and micro‑damage in the plantar fascia. When you take your first step out of bed after a night of rest, the fascia is suddenly stretched from its shortened overnight position, tugging at the inflamed attachment site — that sudden stretch creates the sensation of stepping on a knife.
1.2 Why High Heels and Prolonged Standing Are Major Risk Factors
High heels tilt the foot downward, placing the plantar fascia and Achilles tendon in a continuously shortened position. This static shortening reduces the fascia‘s natural flexibility. When you switch to flat shoes or walk barefoot at home, the tissue must suddenly lengthen, causing micro‑trauma. Over time, the cumulative effect of this daily cycle leads to chronic irritation. Women who wear high heels five days a week and also spend their working hours standing — in retail, hospitality, teaching, healthcare, or office roles that involve long periods on their feet — face a double burden. The combination of static shortening from heel elevation and prolonged weight‑bearing fatigue creates ideal conditions for plantar fasciitis to develop. It is not a coincidence that plantar fasciitis affects approximately 10% of the general population and is notably more common in women.
1.3 Why Morning Pain Is So Much Worse Than Later‑in‑Day Discomfort
During sleep, the feet are typically pointed downward in a relaxed, plantar‑flexed position. In this posture, the plantar fascia shortens and the calf muscles relax. When you suddenly stand and place your full body weight on the foot, the fascia is forced to stretch from its shortened overnight length. If the tissue already has micro‑tears or inflammation, that sudden elongation triggers a sharp, tearing sensation. The pain gradually decreases after a few minutes of walking because gentle movement warms up the tissue, lengthens the fascia, and increases circulation. However, the pain often returns later in the day after prolonged standing or at the end of a long shift when the cumulative fatigue of weight‑bearing has once again irritated the fascia. Understanding this cycle is essential: simply masking the pain without addressing the underlying tissue condition means the same sharp morning step will greet you again tomorrow.
2. How Traditional Patches, Pads, and Pain Pills Work — And Why They Eventually Fail
The pharmacy aisle offers an overwhelming array of products for heel pain. Heating pads, medicated plasters, analgesic gels, and oral painkillers. Each promises relief, yet for many women with chronic plantar fasciitis, the relief is disappointingly short‑lived.
2.1 The Mechanism of Heat‑Activated and Medicated Patches
Heat‑activated patches deliver local warmth that relaxes superficial muscles and temporarily improves circulation to the outer layers of the skin. Medicated plasters containing non‑steroidal anti‑inflammatory drugs release small amounts of medication through the skin, directly to the affected area. Both approaches can reduce superficial inflammation and provide mild analgesic effects. However, the plantar fascia attaches deep within the heel, beneath layers of skin, fat, and muscle. The amount of medication that reaches the actual fascial attachment point through transdermal absorption is limited. Heat, similarly, warms the skin and superficial fat but does not penetrate deeply enough to significantly alter the underlying degenerative or inflammatory process at the fascial insertion. These patches are designed for comfort, not for curing the condition.
2.2 The Limitations of Oral Painkillers for Chronic Heel Pain
Over‑the‑counter oral painkillers work systemically. They circulate through the bloodstream and inhibit pain signals throughout the body. For acute injury, this can be helpful. But for chronic conditions like plantar fasciitis, daily oral medication brings the risk of dose escalation as the body builds tolerance. Long‑term use can also cause gastrointestinal issues — stomach upset, irritation, or even ulcers. More importantly, oral painkillers do absolutely nothing to help the plantar fascia heal. They simply dull the perception of pain while the underlying tissue continues to degenerate. As a result, many women find themselves trapped in a frustrating cycle: they take a painkiller, get through the workday, then wake up the next morning with the same sharp pain. The medication buys temporary comfort but does not buy progress toward recovery.
2.3 Gel Heel Cups, Orthotic Inserts, and Their Place in Treatment
Gel heel cups and cushioned inserts absorb some of the impact during walking, which can reduce the shock transmitted to the painful heel with each step. Custom orthotics may improve foot biomechanics and correct alignment issues that contribute to excessive tension on the plantar fascia. These devices can be helpful as part of a comprehensive management plan, but they rarely eliminate the pain entirely on their own. They address the mechanical environment of the foot without directly healing the damaged tissue. For women who have used heel cups for months with only partial relief, the missing piece is often a therapy that actively stimulates tissue repair rather than merely redistributing pressure.
3. How Extracorporeal Shock Wave Therapy Works for Chronic Heel Pain
Extracorporeal shock wave therapy stands apart from conventional treatments because it does not simply mask pain or alter biomechanics. Instead, it delivers mechanical energy directly to the injured tissue, triggering the body‘s own healing response. For women who have tried patches, pills, and pads without lasting relief, ESWT offers a fundamentally different pathway.
3.1 What Shockwave Therapy Is and How It Reaches the Deep Plantar Fascia
Shockwave therapy involves the application of high‑energy acoustic waves through a handheld device placed against the skin of the painful heel. The waves penetrate through the layers of skin, fat, and muscle to reach the insertion point of the plantar fascia on the calcaneus. At the cellular level, these pressure waves trigger a cascade of biological responses. They increase blood flow to the injured area, stimulate the formation of new blood vessels, promote the release of growth factors, and accelerate collagen production — all essential components of tissue repair. Unlike a painkiller that works on the nervous system, shockwave therapy works directly on the cells of the damaged fascia. It signals the body to shift from a state of chronic degeneration to one of active healing.
3.2 What Clinical Experience Shows About Pain Reduction and Function Improvement
Multiple clinical studies have examined shockwave therapy for chronic plantar fasciitis. A systematic review found that ESWT has been proven to be a successful treatment for the condition, with moderate‑to‑high evidence supporting pain reduction in the short, medium, and long term. Another meta‑analysis concluded that ESWT is superior to ultrasound therapy for plantar fasciitis, particularly in improving pain during activity and overall treatment success rates. When compared to local corticosteroid injections, some research indicates that while injections may provide faster pain relief in the very first weeks, the effect often wears off over time. In contrast, shockwave therapy‘s benefits, although sometimes slower to start, tend to be more durable. A comparative study of corticosteroid injections, shockwave therapy, and radiofrequency ablation found that shockwave therapy provided sustained improvement. A 2025 literature review reaffirmed that ESWT is an effective, valid, and safe method for treating chronic plantar fasciitis. For the woman who has been limping through her workday for months, these findings suggest that a course of shockwave therapy may offer the deeper, more lasting relief that patches and pills cannot provide.
3.3 How ESWT Addresses the Root Cause Rather Than Masking the Symptoms
The fundamental difference between shockwave therapy and conventional treatments lies in the target. Patches and pills target the pain signal — the symptom. They work on the nervous system, not on the damaged tissue. Shockwave therapy targets the tissue itself. The acoustic waves mechanically stimulate the fibroblasts within the plantar fascia, encouraging them to produce new, healthy collagen fibers. The increased blood flow and neovascularization bring oxygen and nutrients to an area that has poor natural blood supply, creating an environment where healing can actually occur. What a woman experiences after a course of shockwave therapy is not merely reduced pain; it is a genuine reduction in the underlying pathology. The morning step that used to feel like stabbing may gradually become a mild tug, then a faint awareness, and finally, nothing at all. The healing is real, not just perceived.
4. Comparing the Two Paths: Temporary Comfort Versus Lasting Relief
For the woman standing in the pharmacy aisle, the decision often comes down to immediate access versus potential long‑term gain. Understanding the difference between these two approaches helps clarify which one aligns with her personal goals.
4.1 The Routine of Daily Self‑Care: Patches, Pills, and Pads
If you choose the conventional path, your daily routine involves remembering to apply a patch before work, taking a painkiller at lunch when the ache worsens, and slipping gel cushions into your shoes each morning. This approach fits neatly into a busy life — no appointments, no co‑payments, no disruption. The problem is that it is a maintenance strategy, not a resolution strategy. Each day, you invest time and money in managing the pain, but the underlying condition does not improve. In fact, over months of masking the pain, the degenerative process may continue or worsen. The daily routine of self‑care becomes a tolerable but frustrating necessity. You learn to live with the pain rather than living without it.
4.2 The Course of Shockwave Treatment: Short‑Term Commitment, Long‑Term Payoff
Shockwave therapy follows a different rhythm. Treatment typically involves three to five sessions, spaced about one week apart. Each session lasts only a few minutes. During the treatment, you may feel a tapping or thumping sensation — uncomfortable for some, but manageable. After the session, you go back to your normal activities immediately. There is no downtime, no bandage, no recovery period. The first few weeks after starting treatment, you might notice that the morning pain is still there, perhaps even temporarily a bit more noticeable as the tissue begins its healing response. But by the fourth to sixth week, many women report that the sharp morning step has become significantly milder. By the end of the course, the pain is often much reduced or even gone. That initial inconvenience of a few appointments pays off with months or years of relief, freeing you from the daily ritual of managing symptoms.
4.3 Why Many Women Eventually Transition from Patches to Shockwave Therapy
Many women do not start with shockwave therapy. They start with patches, pills, and pads because those products are immediately available and require no special appointment. Months or even years later, frustrated by the cycle of temporary relief followed by inevitable return of pain, they begin researching alternatives. They discover that shockwave therapy addresses the condition rather than just the symptom. They weigh the inconvenience of a few appointments against the daily inconvenience of managing pain, and they decide to try something different. The transition from symptomatic management to active treatment is not a failure of the earlier approach — it is a natural progression. The body is trying to heal all along; it simply needs the right stimulus to get started.
5. Building a Strategy That Works for Working Women
For the woman who wears heels to work, stands for hours at a retail counter, and still wants to enjoy her weekends, the ideal treatment plan is not either‑or. It is a thoughtful combination of interventions matched to the stage of her condition.
5.1 When Contemporary Conservative Care Is Appropriate
For very mild, intermittent heel pain, conservative measures are a reasonable starting point. Rest, supportive footwear, heel cups, and occasional use of topical pain relievers may be enough to calm the inflammation. If the pain appears only after unusually long days on your feet and resolves with a good night‘s sleep, a patch or a padded insole may represent a cost‑effective, low‑risk strategy. The key is recognizing when conservative care is no longer sufficient — when the pain returns every morning, when you wake up dreading that first step, when you find yourself avoiding activities you used to enjoy.
5.2 When to Consider Shockwave Therapy
Shockwave therapy should be considered when heel pain has persisted for many weeks despite consistent use of conservative measures, when the pain interferes with daily activities, or when you find yourself taking painkillers on a regular basis just to get through the day. It is also a strong option for women who want to avoid corticosteroid injections — which carry a small risk of plantar fascia rupture and fat pad atrophy — or who are not candidates for surgery. The therapy is well‑tolerated, non‑invasive, and does not require you to interrupt your work schedule. For the busy professional with a full calendar, the ability to schedule a brief appointment and return directly to the office is a practical benefit that should not be underestimated.
5.3 The Complementary Role of Supportive Footwear and Stretching
Even the most effective shockwave therapy will struggle to maintain its benefits if the mechanical stresses that caused the condition in the first place are not addressed. That is why the best long‑term strategy combines active treatment with sensible daily habits. Wear shoes with adequate arch support and cushioning, not only at work but also around the house. Avoid walking barefoot on hard floors, especially in the morning before the fascia has had a chance to warm up. Perform gentle calf stretches before getting out of bed — pulling the toes toward the shin using a towel or your hands — to lengthen the fascia before weight‑bearing. These simple habits do not replace shockwave therapy, but they extend and protect its results. Together, they form a complete approach to keeping your feet happy for years to come.
FAQ
Q1: Does shockwave therapy for heel spurs hurt during the procedure?
Most people describe the sensation as a strong tapping or deep thumping. Some discomfort is normal, but the intensity can be adjusted to remain manageable.
Q2: How soon will I notice less morning pain after starting shockwave therapy?
Many women notice a reduction in sharp morning pain after the second or third session. Full improvement often becomes apparent several weeks after completing the treatment course.
Q3: Can I continue wearing high heels while undergoing shockwave therapy?
It is best to minimize heel height during treatment and limit prolonged standing when possible. Supportive, cushioned footwear supports the healing process.
Q4: How many shockwave sessions will I need for chronic heel pain?
Most patients benefit from three to five sessions spaced about one week apart. Some may need a second course after several months.
Q5: Will I need to use pain patches or pills after completing shockwave therapy?
Many women find that after a successful course of shockwave therapy, they no longer need daily pain medications or patches. The goal is lasting relief, not ongoing symptom management.
الخاتمة
The morning alarm that once announced a sharp, stabbing pain in your heel does not have to define your day. For the woman who wears high heels to work, stands on her feet for hours, and refuses to let heel pain steal her joy, the choice is not between suffering and daily medication. There is a third path. Extracorporeal shock wave therapy offers a non‑invasive, drug‑free way to help the plantar fascia heal from within, addressing the root cause of the pain rather than just quieting the symptom. Patches and pills have their place, but they are a temporary companion for a chronic condition when used alone. Shockwave therapy is a commitment to long‑term relief — a few appointments for the sake of waking up without dread. You can step out of bed without hesitation, walk through your workday without limping, and enjoy the weekend without wincing. Your feet have carried you through life; with the right care, they can carry you through many more years of pain‑free steps.
المراجع
Back2HealthTN. Laser Therapy for Plantar Fasciitis.
Medimarket. Shockwave Therapy for Heel Pain.
Dynamic Chiropractic. Shockwave Therapy for Chronic Plantar Fasciitis.
https://dynamicchiropractic.com
Megan Wolf MD. Shockwave Treatment for Plantar Fasciitis.
Axis Sports Med. Shockwave Therapy – No Pain, No Gain?