
Introduction
The daily rhythm of a professional kitchen involves repetitive gripping, lifting, stirring, and wrist extension. These motions, performed hundreds of times each shift, place exceptional mechanical stress on the tendons around the elbow. Many chefs accept elbow pain as an unavoidable part of the job, pushing through the discomfort until it interferes with basic tasks like lifting a pot or gripping a knife. What they are experiencing is likely lateral epicondylitis—commonly known as tennis elbow—but without the tennis. This tendinopathy stems from degenerative changes within the tendon rather than acute inflammation, which explains why rest alone rarely provides lasting relief. Extracorporeal shockwave therapy (ESWT) offers a non-invasive, drug-free approach that targets the underlying tissue degeneration, potentially helping chefs return to their craft without extended time away from the kitchen.
1. The Chef‘s Elbow: Understanding Occupational Lateral Epicondylitis
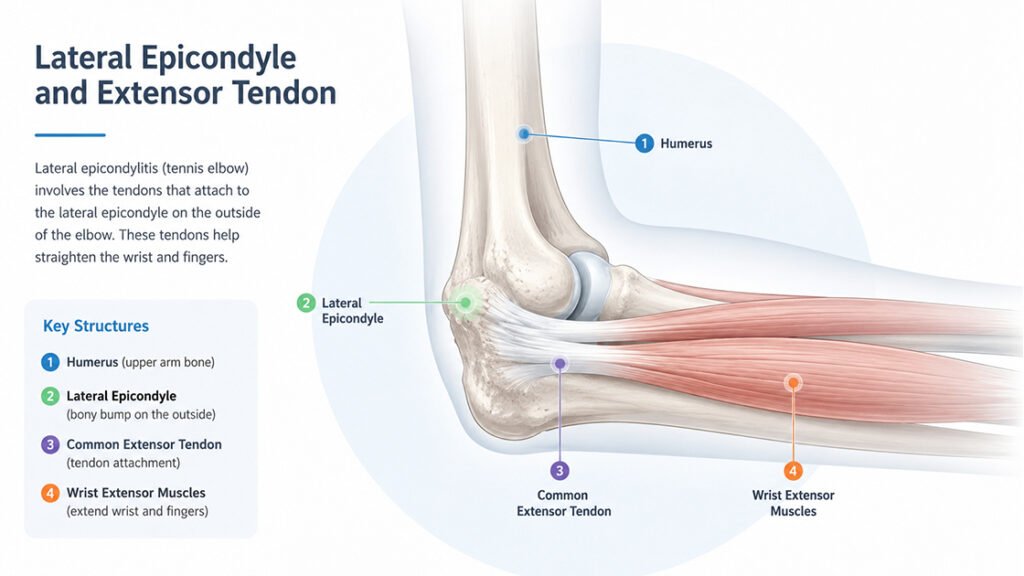
Lateral epicondylitis affects the common extensor tendon, which attaches to the lateral epicondyle of the humerus—the bony bump on the outer side of the elbow. This tendon anchors the muscles that extend the wrist and fingers, movements essential for nearly every kitchen task. When chefs repeatedly grip heavy pans, stir thick sauces, or lift large stockpots, the extensor muscles contract forcefully, transmitting high tensile loads through the tendon attachment. Over time, microscopic injuries accumulate faster than the body can repair them, leading to degenerative changes within the tendon structure rather than the classic inflammation that the suffix “-itis” suggests.
1.1 Prevalence Among Kitchen Professionals
Studies examining the culinary workforce reveal consistently high rates of lateral epicondylitis. A cross-sectional study of 200 chefs found that more than two-thirds tested positive for lateral epicondylitis using clinical provocation maneuvers that reproduce pain at the lateral epicondyle. Chefs aged 30 to 34 showed the highest frequency, and longer working hours correlated significantly with positive test results. Another study reported a similar prevalence among restaurant cooks, with most working more than eight hours per day. Research examining functional disability found that more than one-third of chefs with lateral epicondylitis reported that their elbow pain significantly interfered with daily activities, work performance, and recreation.
1.2 Repetitive Load as the Primary Driver
The kitchen environment creates a perfect storm of risk factors for elbow tendinopathy. Chefs perform high-repetition gripping and wrist extension tasks throughout each shift, often with the elbow positioned at angles that maximize tendon tension. Lifting heavy pots, stirring dense mixtures, and chopping ingredients require sustained muscle contraction that reduces blood flow to the tendon, limiting the delivery of oxygen and nutrients needed for tissue maintenance. The cumulative effect of these daily mechanical demands explains why lateral epicondylitis ranks as one of the most common work-related musculoskeletal disorders among culinary professionals.
2. From Tendon Strain to Tendinopathy
Understanding how a healthy tendon becomes a painful, dysfunctional one requires a closer look at the tissue‘s biology. Tendons transmit force from muscle to bone, and their specialized structure—dense bundles of collagen fibers arranged in parallel—provides the tensile strength needed for this role. However, this structure also limits blood supply. Poor vascularity means tendons rely heavily on diffusion for nutrient exchange, making them slow to adapt to increased mechanical demands.
2.1 The Degenerative Process
When chefs perform thousands of gripping and lifting repetitions week after week, the cumulative tensile load on the common extensor tendon begins to exceed the tissue‘s adaptive capacity. Microtears develop at the cellular level, particularly within the origin of the extensor carpi radialis brevis, the deepest of the wrist extensor muscles. In a healthy tendon, repair mechanisms would quickly address these minor injuries. But the repetitive nature of kitchen work keeps the tendon under continuous stress, disrupting the normal balance between breakdown and repair. Over months or years, this imbalance leads to degenerative tendinopathy characterized by disorganized collagen, increased ground substance, and the formation of new blood vessels and nerve fibers within the tendon.
2.2 Why Rest Alone Often Fails
Many chefs assume that a few days off will resolve their elbow pain. When the tendon has undergone true degenerative change, however, rest provides only temporary relief because the structural abnormalities remain. The tendon does not need anti-inflammatory treatment—it needs remodeling. The disorganized collagen must be replaced with properly aligned fibers, and the abnormal nerve ingrowth that contributes to pain must be addressed. This understanding has shifted treatment away from passive rest and anti-inflammatory medications toward interventions that actively stimulate tissue repair.
3. How Shockwave Therapy Works at the Cellular Level
Extracorporeal shockwave therapy delivers high-energy acoustic pulses through the skin to the injured tendon. These pressure waves travel through soft tissues and concentrate their energy at the tendon attachment site. The mechanical input triggers a cascade of biological responses that promote healing, not by reducing inflammation, but by stimulating the body‘s own repair mechanisms.
3.1 Mechanotransduction and Cellular Activation
When shockwaves reach the degenerative tendon, the mechanical energy stretches and compresses cells in ways that activate mechanotransduction pathways. Tenocytes—the specialized cells within the tendon—respond to this mechanical stimulus by increasing their production of growth factors and signaling molecules. This activation shifts the tendon from a quiescent, degenerative state toward an active repair phase. The mechanical input also releases biologically active molecules from the extracellular matrix, further amplifying the healing signal.
3.2 Neovascularization and Improved Perfusion
Degenerative tendons typically show reduced blood flow at the injury site, a factor that perpetuates poor healing. ESWT stimulates the formation of new capillary networks around the treated tendon. This process, known as neovascularization, gradually improves local blood supply. Better perfusion brings oxygen and nutrients to the tenocytes, supports the removal of metabolic waste, and creates an environment more conducive to tissue remodeling.
3.3 Collagen Remodeling and Matrix Restoration
The hallmark of chronic tendinopathy is disorganized collagen that lacks the mechanical strength of healthy tendon tissue. ESWT influences collagen metabolism by stimulating tenocyte proliferation and promoting the synthesis of new collagen fibers. Over the weeks following treatment, the new collagen gradually aligns along lines of mechanical tension, restoring some of the tendon‘s original tensile properties. This remodeling process does not happen overnight, which explains why the full effects of shockwave therapy often take several weeks to appear.
4. Clinical Evidence for Lateral Epicondylitis
A substantial body of research supports the use of shockwave therapy for lateral epicondylitis. Randomized controlled trials and systematic reviews have examined both pain reduction and functional improvement, providing guidance on what patients can reasonably expect.
4.1 Comparison with Corticosteroid Injections
Corticosteroid injections remain a common treatment for tennis elbow, offering rapid pain relief. However, the long-term picture tells a different story. A systematic review and meta-analysis comparing ESWT with local corticosteroid injection for chronic lateral epicondylitis found that corticosteroid injections produced better outcomes at one month, but ESWT showed superior results for pain relief and functional recovery at three months and six months. Another study reported that ESWT achieved a very high success rate at six-month follow-up with no recurrence, whereas the corticosteroid injection group showed a notable recurrence rate over the same period. These findings suggest that while steroids offer faster initial relief, shockwave therapy provides more durable improvement.
4.2 Effectiveness Compared to Other Modalities
A randomized clinical trial comparing ESWT with ultrasound therapy combined with deep friction massage found that both interventions improved pain and function, but between-group analysis revealed that ESWT was significantly more effective than the combined approach. Another randomized controlled trial comparing focused shockwave therapy with ultrasound therapy for lateral epicondylitis found that pain reduction and functional improvement were significantly greater after shockwave therapy. The evidence consistently positions ESWT as an effective non-surgical option for persistent elbow tendinopathy.
4.3 Energy Level Considerations
The optimal energy level for treating lateral epicondylitis remains an area of active investigation. A retrospective study of patients with chronic lateral epicondylitis compared low-energy ESWT with high-energy ESWT, with both groups receiving three weekly sessions. At three months and six months post-treatment, the low-energy group showed significantly greater reductions in pain scores and greater functional improvement. These findings suggest that higher energy does not necessarily yield better outcomes and that appropriate energy selection matters.
5. Integrating Shockwave Therapy into a Comprehensive Approach
Shockwave therapy works most effectively when chefs also address the factors that contributed to their elbow tendinopathy in the first place. The treatment supports tissue healing, but maintaining that improvement requires adjustments to daily kitchen routines.
5.1 Ergonomic Modifications in the Kitchen
Small changes in equipment and technique can meaningfully reduce tendon load. Using heavier knives with larger handles reduces the grip force needed for cutting tasks. Selecting lighter pots and pans for frequent lifting decreases the tensile load on the extensor tendon. Adjusting work surface heights to elbow level minimizes wrist extension during chopping and stirring. Taking brief micro-breaks between tasks allows the tendon to unload briefly, interrupting the cycle of continuous strain.
5.2 Complementary Self-Care Strategies
When chefs can modify their tool usage and work patterns, the elbow tendon experiences fewer insults that undermine healing. This supportive approach includes gradually reintroducing demanding tasks rather than returning to full kitchen duties immediately after treatment. Spreading heavy lifting and high-repetition tasks throughout the shift rather than concentrating them in short periods helps distribute mechanical loads more evenly. These adjustments create a more favorable mechanical environment for the tendon to respond to the biological stimulus provided by shockwave therapy.
FAQ
Q1: Is shockwave therapy painful for elbow tendinopathy?
Most chefs describe a tapping or sharp sensation at the treatment site that is uncomfortable but tolerable. The session lasts only a few minutes, and discomfort stops when the probe lifts.
Q2: How many sessions does a chef typically need?
A common protocol involves three sessions spaced about one week apart. Some chefs notice improvement after the first session, while the full effect often becomes apparent over the following weeks.
Q3: Can a chef keep working during shockwave therapy?
Yes, most chefs continue their regular duties during treatment. Avoiding the specific movements that aggravate the elbow may help support the healing response.
Q4: How long before a chef feels improvement?
Some chefs notice reduced pain within a few days, but the most noticeable improvement typically appears four to six weeks after completing the treatment series as the tendon remodels.
Q5: Does shockwave therapy work for both elbows?
Yes, when both elbows are affected, each side can be treated separately. Bilateral involvement occurs in a notable percentage of chefs with elbow tendinopathy.
Conclusion
Professional chefs develop elbow tendinopathy not from weekend sports but from the relentless demands of daily kitchen work. The repetitive gripping, lifting, and stirring that define culinary practice place exceptional strain on the common extensor tendon, leading to degenerative changes that rest alone cannot reverse. For chefs who have tried ice, braces, and time off without lasting relief, extracorporeal shockwave therapy offers a non-invasive, drug-free approach that addresses the underlying tissue degeneration. By stimulating neovascularization, activating tenocyte repair mechanisms, and promoting collagen remodeling, ESWT supports the body‘s own healing processes. When combined with sensible ergonomic adjustments in the kitchen, shockwave therapy can help chefs return to their craft with less pain and greater confidence.
References
Prevalence of Lateral Epicondylitis among Chefs and Its Association with Age, Gender, and Working Hours
https://jnah.supp.journalrmc.com/index.php/public/article/view/128
Prevalence and Risk Factors of Lateral Epicondylitis among Restaurant Cooks
Impact of Tennis Elbow on Functional Disability and Physical Therapy Awareness among Chefs
https://www.pakjr.com/index.php/PJR/article/view/1848
High Versus Low-Energy Extracorporeal Shockwave Therapy for Chronic Lateral Epicondylitis: A Retrospective Study
https://pmc.ncbi.nlm.nih.gov/articles/PMC11432994
Extracorporeal Shock Wave Therapy Versus Local Corticosteroid Injection for Chronic Lateral Epicondylitis: A Systematic Review with Meta-Analysis
https://discovery.ebscomedical.com/eds/detail?db=a9h&an=180737084
Focused Shock Wave and Ultrasound Therapies in the Treatment of Lateral Epicondylitis
https://www.nature.com/articles/s41598-024-77410-w
Effects of Extracorporeal Shockwave Therapy versus Ultrasonic Therapy and Deep Friction Massage in the Management of Lateral Epicondylitis
https://link.springer.com/article/10.1038/s41598-024-67313-1
Extracorporeal Shockwave Therapy versus Steroid Injection in Treatment of Tennis Elbow