
Understanding Calcific Tendonitis
Calcific tendonitis is a musculoskeletal disorder characterized by the deposition of calcium hydroxyapatite crystals within tendons, most commonly affecting the rotator cuff of the shoulder. This condition progresses through distinct phases:
- Pre-calcific phase: Tendon cells undergo fibrocartilaginous metaplasia, often asymptomatic.
- Calcific phase: Calcium deposits form within the tendon, which may or may not cause symptoms.
- Resorptive phase: The body initiates an inflammatory response to reabsorb the calcium, leading to acute pain.
- Post-calcific phase: Healing occurs with remodeling of the tendon tissue.
Diagnosis involves:
- X-rays: Reveal calcific deposits within the tendons.
- Ultrasound: Assesses the size and consistency of the deposits and evaluates tendon integrity.
- MRI: Provides detailed images of soft tissue structures, useful in complex cases.

Why Traditional Treatments Often Fall Short
Ice and NSAIDs: A Temporary Fix
Nonsteroidal anti-inflammatory drugs (NSAIDs) and cryotherapy are commonly used to alleviate pain and inflammation in calcific tendonitis. While they may provide short-term relief, they do not address the underlying calcium deposits. Prolonged use of NSAIDs can lead to gastrointestinal, renal, and cardiovascular side effects.
Physical Therapy: Slow Results for a Stubborn Condition
Physical therapy (PT) focuses on restoring range of motion and strengthening the rotator cuff muscles. Techniques include:
- Eccentric exercises: Shown to be effective in managing tendinopathies.
- Manual therapy and stretching: Aims to improve flexibility and reduce pain.
However, PT may require several months to yield significant improvements, and its efficacy in resolving calcific deposits is limited.
Steroid Injections: Relief with Side Effects
Corticosteroid injections can reduce inflammation and provide pain relief. Nevertheless, their benefits are often transient, and repeated injections may weaken tendon structure, increasing the risk of rupture. Additionally, they do not facilitate the resorption of calcium deposits.
Surgery: When It Feels Like the Only Option
Surgical intervention, such as arthroscopic removal of calcium deposits, is considered when conservative treatments fail. While surgery can effectively eliminate deposits and alleviate symptoms, it carries inherent risks, including infection, anesthesia complications, and prolonged rehabilitation periods. Moreover, surgery addresses the symptoms but not the underlying pathophysiological processes that lead to calcific tendonitis.
Beating Calcific Tendonitis with Sound Waves
What Is Shockwave Therapy?
Extracorporeal Shockwave Therapy (ESWT) is a non-invasive treatment modality that utilizes acoustic waves to stimulate healing in musculoskeletal conditions, including calcific tendonitis. These high-energy sound waves are transmitted through the skin to the affected tendon, promoting tissue regeneration and pain relief. ESWT is categorized into two main types: Focused Shockwave Therapy (FSWT) and Radial Shockwave Therapy (RSWT). FSWT delivers energy to a specific depth, making it suitable for targeting deep-seated calcifications, while RSWT disperses energy over a broader area, often used for superficial lesions.

How It Targets Calcium Deposits
In calcific tendonitis, calcium hydroxyapatite crystals accumulate within the tendon, leading to pain and inflammation. Shockwave therapy addresses this by inducing mechanical stress and cavitation effects that fragment the calcium deposits. This fragmentation facilitates the body’s natural resorption processes, gradually eliminating the calcific buildup. Additionally, ESWT enhances neovascularization and stimulates the release of growth factors, further supporting tendon healing.
High-Energy vs. Low-Energy Shockwave
The efficacy of ESWT can vary based on the energy levels used:
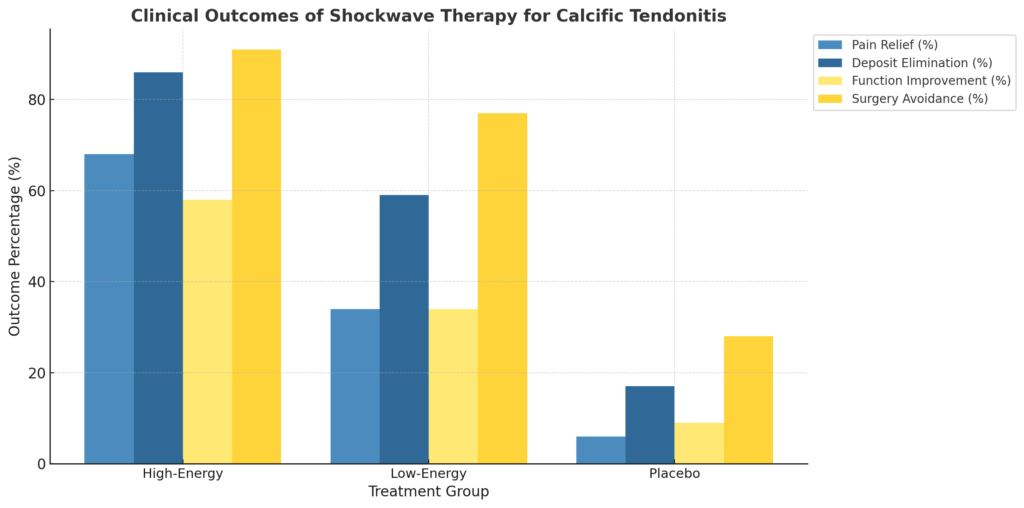
- High-Energy ESWT: Characterized by an energy flux density (EFD) typically above 0.28 mJ/mm², high-energy treatments have demonstrated superior outcomes in dissolving calcium deposits and improving shoulder function. A meta-analysis indicated that patients receiving high-energy ESWT experienced greater improvements in the Constant-Murley score compared to those receiving low-energy treatments.
- Low-Energy ESWT: With EFDs below 0.12 mJ/mm², low-energy treatments are generally better tolerated but may require more sessions to achieve comparable results. While effective in reducing pain and improving function, their impact on calcific resorption is less pronounced than high-energy treatments.
How Fast Does Shockwave Therapy Work for Calcific Tendonitis?
The timeline for symptom relief and functional improvement varies among individuals. Clinical studies have reported significant pain reduction and enhanced mobility within 3 to 6 weeks post-treatment. A typical ESWT regimen involves 3 to 6 sessions, spaced one week apart, allowing the tendon to respond and heal between treatments . Factors influencing the rate of improvement include the size and density of the calcium deposit, the chronicity of the condition, and the patient’s overall health status.
Proven Benefits of Shockwave Therapy for Tendon Healing
Breaks Down Calcium Deposits
ESWT effectively disintegrates calcific deposits within tendons. A study reported that 57.6% of patients achieved complete dissolution of calcium deposits following shockwave therapy, with an additional 15.1% experiencing partial resorption . This mechanical disruption facilitates the body’s natural clearance mechanisms, reducing the source of inflammation and pain.
Stimulates Natural Tendon Regeneration
Beyond mechanical effects, shockwave therapy promotes biological healing processes. It stimulates angiogenesis—the formation of new blood vessels—and the release of growth factors such as endothelial nitric oxide synthase (eNOS) and vascular endothelial growth factor (VEGF). These factors enhance blood flow and cellular activity, accelerating tendon repair and regeneration.
Reduces Pain and Inflammation Quickly
Patients often experience rapid pain relief following ESWT. The therapy modulates nociceptor activity and reduces the concentration of substance P, a neuropeptide associated with pain transmission. This neurochemical modulation, combined with decreased inflammation from calcific breakdown, contributes to swift symptom alleviation.
Improves Mobility Without Downtime
As a non-invasive procedure, shockwave therapy allows patients to resume daily activities shortly after treatment. Unlike surgical interventions, ESWT does not require anesthesia or extended recovery periods, minimizing disruption to the patient’s routine. Improved tendon function and reduced pain contribute to enhanced joint mobility and quality of life.
Long-Term Effectiveness: Does It Prevent Recurrence?
Long-term studies indicate that shockwave therapy not only provides immediate relief but also sustains improvements over time. One study reported a recurrence rate of only 6.5% over a two-year follow-up period, suggesting durable benefits . The combination of mechanical and biological effects of ESWT addresses both symptoms and underlying pathology, reducing the likelihood of recurrence.
What to Expect During and After a Shockwave Session
What a Typical Session Looks Like
A standard Extracorporeal Shockwave Therapy (ESWT) session for calcific tendonitis typically lasts between 15 to 30 minutes. During the procedure, the patient is positioned comfortably, and the treatment area is identified using palpation or imaging techniques. A coupling gel is applied to the skin to facilitate efficient transmission of shockwaves. The clinician then administers shockwaves using a handheld applicator, delivering a predetermined number of impulses (usually between 1,500 to 3,000) at a specific energy flux density (EFD). The choice between focused or radial shockwave devices depends on the depth and size of the calcific deposit.
Does It Hurt? Side Effects to Know
Patients may experience mild to moderate discomfort during the procedure, often described as a tapping or pulsing sensation. Post-treatment side effects are generally minimal but can include:
- Pain or discomfort: Transient soreness at the treatment site.
- Erythema and swelling: Temporary redness or swelling due to increased blood flow.
- Ecchymosis: Minor bruising in the treated area.
- Paresthesia: Tingling sensations that typically resolve within a few days.
These side effects are usually self-limiting and resolve within a week. Serious adverse events are rare when ESWT is performed by trained professionals.
How Many Sessions Are Needed?
The number of ESWT sessions required varies based on the severity and chronicity of the calcific tendonitis. Typically, patients undergo a series of 3 to 5 sessions, spaced one week apart. Some cases may necessitate additional treatments to achieve optimal outcomes. Clinical studies have demonstrated significant improvements in pain and function after completing the treatment course.
Post-Treatment Care and Activity Guidelines
After an ESWT session, patients are generally advised to:
- Rest the treated area: Avoid strenuous activities for 48 hours post-treatment.
- Apply ice if needed: Use cold packs to alleviate any discomfort or swelling.
- Avoid anti-inflammatory medications: NSAIDs may interfere with the body’s natural healing response; consult with a healthcare provider before use.
- Engage in prescribed exercises: Follow a tailored rehabilitation program to enhance recovery and prevent recurrence.
Adherence to post-treatment guidelines is crucial for maximizing the benefits of ESWT and ensuring a smooth recovery process.
Real Stories, Real Results: Testimonials and Case Studies
Patient Testimonials Reflecting Real-World Impact
“My orthopedist recommended shockwave therapy after months of failed NSAIDs and physical therapy. After four sessions, the ultrasound confirmed a 70% reduction in my calcific deposit. I avoided surgery and regained 90% of my shoulder mobility.”
“After three ESWT sessions, my pain dropped from an 8 to a 2 on the VAS scale. My supraspinatus tendon calcification nearly disappeared by the fifth week.”
“The results were gradual, but dramatic. Not only did my ROM improve, but post-treatment imaging showed calcium disintegration. I was able to avoid invasive procedures altogether.”
Peer-Reviewed Case Studies and Clinical Outcomes
Case Study: Efficacy of ESWT in Treating Calcific Tendonitis of the Shoulder
Objective: Evaluate the clinical effect of radial shockwave therapy (rESWT) on patients with chronic calcific tendinitis of the supraspinatus tendon.
Sample Size: 30 patients aged 35–65 years with radiologically confirmed Type I and II calcific deposits.
Protocol:
- Device Used: Radial ESWT (2.0 bar pressure)
- Pulse Count: 2,000 pulses per session
- Frequency: Once weekly for 3 weeks
Outcome Measures:
- Visual Analogue Scale (VAS) for pain
- Shoulder Pain and Disability Index (SPADI)
- Ultrasound Imaging for calcific deposit measurement
Results:
- VAS Pain Score: Reduced from a mean of 7.3 to 3.0 after 3 weeks (≈ 58.9% reduction)
- SPADI Function Score: Improved from 68% disability to 39% (≈ 42.6% functional gain)
- Ultrasound Evaluation: Showed partial or full resorption of calcium in 76.6% of patients
- Clinical Note: Patients reported improved range of motion (ROM) and lower reliance on analgesics.
Learn about Contraindications of Shockwave Therapy
While shockwave therapy (ESWT) is safe and non-invasive, certain medical conditions and situations require caution or absolute contraindication.
Absolute Contraindications
- Pregnancy: Risk to fetal development from energy transmission.
- Malignancy: Avoid treating near tumor sites to prevent metastasis stimulation.
- Active Infections or Open Wounds: Especially over the treatment area.
- Severe Coagulopathy or Blood Disorders: e.g., hemophilia, or patients on anticoagulants like warfarin.
Relative Contraindications (Use with Caution)
- Pacemakers or Implantable Devices: Risk of interference from energy fields.
- Epiphyseal Plates in Children: May affect bone growth.
- Neuropathic Disorders: Patients with impaired sensation may not perceive discomfort or injury during treatment.
- Uncontrolled Diabetes: Delayed healing response; should be carefully monitored.
References
Arthroscopy surgery versus shock wave therapy for chronic calcifying tendinitis of the shoulder:
https://pmc.ncbi.nlm.nih.gov/articles/PMC2657331
Applying Focused and Radial Shock Wave for Calcific Tendinitis of the Shoulder : Randomized Controlled Study:
https://www.jptrs.org/journal/view.html?doi=10.14474/ptrs.2022.11.3.356