
Introduction
The body weight pressing through the palms, wrists bent back at an angle, breath steady as the pose holds. For yoga and Pilates instructors, these moments define both their teaching and their personal practice. Yet the movements that build strength and flexibility also place unique demands on a joint designed more for mobility than for sustained weight‑bearing. Many instructors accept occasional wrist soreness as part of the profession. However, persistent discomfort on the back of the hand where the fingers meet the wrist may signal something more specific than ordinary fatigue. This discomfort can stem from carpal bossing—a bony protuberance at the base of the second or third metacarpal—or from the broader pattern of wrist overload syndrome, where repetitive hyperextension and compressive loading irritate the dorsal soft tissues. Extracorporeal shockwave therapy (ESWT) offers a non‑invasive, drug‑free approach that may help manage wrist discomfort while allowing instructors to continue sharing their craft.
1. Understanding Wrist Overload in Yoga and Pilates
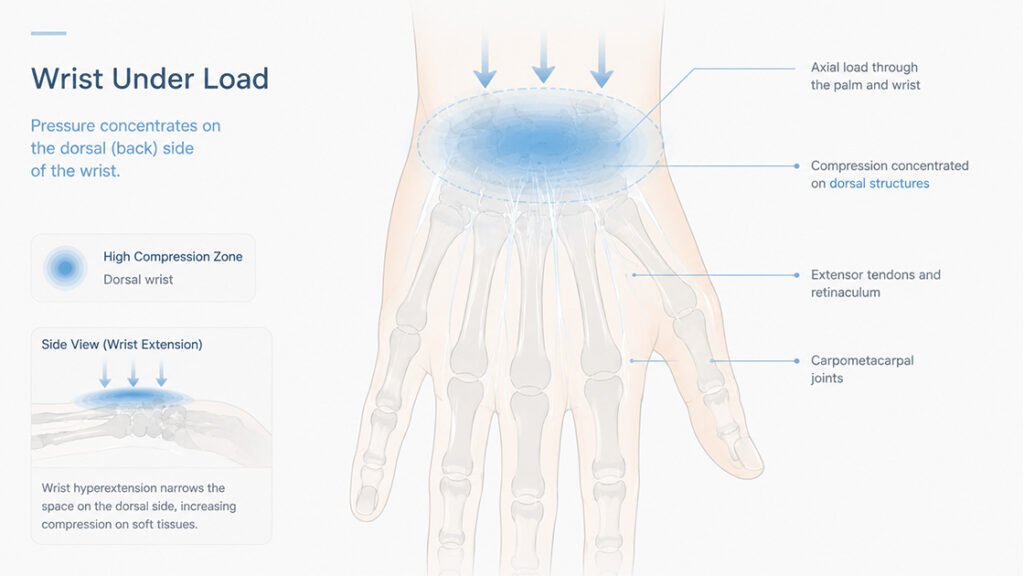
The wrist joint balances remarkable mobility with reasonable stability, but it was not primarily designed to bear the full weight of the human body for extended periods. In yoga asanas such as Downward‑Facing Dog, Plank, or Crow Pose, the wrist assumes a position of hyperextension—bent backward beyond its neutral alignment—while supporting a significant portion of body weight. Pilates exercises on the reformer or mat that involve weight‑bearing through the hands place similar demands. Over time, this repeated loading pattern can create a cascade of mechanical and biological changes in the dorsal (back) aspect of the wrist.
1.1 The Anatomy Under Pressure
When the wrist hyperextends during weight‑bearing, the carpal bones shift slightly, and the soft tissues on the dorsal side—including the extensor tendons, their retinaculum, and the joint capsules—become compressed between the bony structures and the ground. The extensor carpi radialis brevis and longus, which run along the back of the hand and wrist, experience increased friction as they glide over the underlying carpometacarpal joints. Prolonged or repetitive loading in this position can irritate these tendons, leading to an aching or sharp sensation localized near the base of the index or middle finger. For many instructors, the deep crease of the wrist may also show signs of prolonged pressure, with the skin becoming calloused or sensitive to touch.
1.2 Why Some Instructors Experience More Discomfort
Not everyone who practices yoga or Pilates develops persistent wrist discomfort, but certain anatomical variations and practice habits increase susceptibility. Individuals with hyperflexible joints may extend their wrists beyond the range that their supporting ligaments can comfortably manage, placing additional strain on the capsule and tendons. Instructors who teach multiple classes daily without sufficient recovery time may experience cumulative microtrauma that exceeds the tissues‘ adaptive capacity. Additionally, a phenomenon known as carpal bossing involves a bony protuberance at the base of the index or middle finger metacarpal. In most people this remains asymptomatic, but under repeated hyperextension loading, the bony prominence can press against overlying extensor tendons, producing pain during or after weight‑bearing poses.
2. Carpal Bossing: When a Silent Anatomical Variant Becomes Symptomatic
A significant percentage of the population carries a bony bump on the back of their wrist without ever knowing it. Anatomical studies report that a carpal boss—a bony protuberance at the dorsal aspect of the joint involving the base of the second and third metacarpal bones—exists in many individuals. Yet only a small fraction of those ever develop symptoms. The rising popularity of weight‑bearing wrist postures in yoga and Pilates appears to convert some of those silent anatomical variants into symptomatic ones.
2.1 Mechanism of Impingement
In a person with a carpal boss, the bony prominence sits normally without causing trouble. But when the wrist hyperextends under load, that protruding bone can press against the overlying extensor tendons and the dorsal capsule of the carpometacarpal joint. This impingement produces pain not necessarily during the activity itself, but often afterward or in specific loaded positions. Some instructors may notice a hard, immovable swelling on the back of their hand at the base of the index or middle finger that becomes more apparent when they flex the wrist. Pressing on that spot reproduces the familiar ache. The pain may also radiate locally, sometimes confusing the clinical picture.
2.2 Beyond the Bony Bump
Not all wrist discomfort in yoga and Pilates instructors traces back to a carpal boss. Some instructors experience symptoms from extensor tendinopathy, where the tendons themselves become irritated without an underlying bony prominence. Others may develop dorsal wrist ganglion cysts, soft tissue swellings that can accompany or even mask the presence of a carpal boss. In some cases, the interface between the extensor retinaculum and the underlying bone becomes chronically inflamed, leading to a condition known as dorsal wrist impingement syndrome. Regardless of the precise source, the common thread is repetitive hyperextension loading that exceeds the tissue’s ability to maintain comfort.
3. How Shockwave Therapy Interacts with Wrist Tissues
Extracorporeal shockwave therapy delivers high‑energy acoustic pulses through the skin to deeper structures. For wrist overload conditions, the applicator can be positioned over the dorsal aspect of the hand, targeting the region where the carpal boss, extensor tendons, or joint capsule lies. The mechanical energy from the shockwaves triggers biological responses that support tissue recovery.
3.1 Mechanotransduction and Cellular Activation in Shockwave Therapy
When shockwaves reach the target area, the mechanical pressure stretches and compresses cells in ways that activate mechanotransduction pathways. Fibroblasts and tenocytes respond by increasing their production of growth factors and signaling molecules. This activation shifts the local environment from a state of chronic irritation toward a more active repair phase. The mechanical input also releases biologically active molecules from the extracellular matrix, further amplifying the healing signal without introducing any foreign substance. This process is central to how shockwave therapy influences tissue recovery without pharmaceuticals.
3.2 How Shockwave Therapy Improves Local Blood Flow
Chronic overuse conditions often involve reduced microcirculation in the affected tissues. Poor blood flow limits the delivery of oxygen and nutrients needed for tissue maintenance. Shockwave therapy stimulates the formation of new capillary networks around the treated area, a process called neovascularization. Better perfusion brings healing cells and factors to the irritated tendons or capsules while removing metabolic waste products that can accumulate with repetitive loading. This vascular response is one reason shockwave therapy may benefit instructors with ongoing wrist discomfort.
3.3 Pain Modulation and Tendon Gliding via Shockwave Therapy
The analgesic effects of shockwave therapy involve modulation of nerve signaling. The mechanical energy can alter how pain receptors transmit signals to the central nervous system, providing a period of reduced discomfort. Additionally, by helping to break down small adhesions or soften fibrotic tissue around the extensor tendons, shockwave therapy may improve the smooth gliding of tendons over the underlying bony prominences. This can reduce the friction that contributes to the sensation of catching or pain during wrist extension.
4. What to Expect from Shockwave Therapy for Wrist Overload
For yoga and Pilates instructors considering shockwave therapy, understanding the typical course of treatment helps set realistic expectations. The therapy is not an immediate fix but rather a process that supports the body‘s own healing over several weeks.
4.1 Number of Sessions and Timing for Shockwave Therapy
A common protocol for chronic tendinopathy or impingement involves three to five sessions spaced about one week apart. Each session lasts only a few minutes, with the applicator moved over the dorsal wrist. Most instructors find the sensation—often described as a tapping or sharp pressure—tolerable for the brief duration. Some notice a mild increase in soreness for a day or two after the first session, followed by gradual improvement. The full benefit typically becomes apparent several weeks after completing the series, as tissue remodeling takes time.
4.2 What the Sensation Feels Like During Shockwave Therapy
The shockwave applicator transmits acoustic pulses that travel through skin and soft tissue. Many people describe the feeling as a series of firm taps or a deep percussion. The intensity can be adjusted, and the practitioner typically starts with lower energy, increasing gradually based on comfort. Unlike electrical stimulation, shockwave does not cause muscle contraction. The discomfort, if any, stops as soon as the applicator lifts. For the dorsal wrist, which has relatively little soft tissue padding, the sensation may be more noticeable than over larger muscle groups, but most instructors tolerate it well.
4.3 Combining Shockwave Therapy with Practice Modifications
Shockwave therapy works most effectively when instructors also adjust how they load their wrists during practice. Using wedges or blocks to reduce the angle of wrist extension, distributing weight across the entire hand rather than concentrating it on the heel of the palm, and incorporating wrist‑strengthening exercises can all complement the effects of shockwave therapy. The goal is not to eliminate weight‑bearing entirely but to create a mechanical environment that gives the irritated tissues a chance to recover.
5. Integrating Shockwave Therapy into a Long‑Term Wrist Care Plan
Managing wrist overload requires more than occasional treatment. Instructors who maintain healthy wrists over years of teaching adopt habits that reduce cumulative strain.
5.1 Warm‑Up and Cool‑Down Routines
A few minutes of gentle wrist circles, flexion‑extension movements, and light stretching before practice can improve tissue pliability. After teaching, applying a cool compress or simply shaking out the hands helps signal the tissues that the loading period has ended. Instructors who rush from the last pose to the next task without this transition may carry residual tension into their daily activities.
5.2 Strengthening Supporting Muscles
Strong forearms and hands take some load off the wrist joint itself. Simple exercises such as wrist curls with light resistance, finger extensions using rubber bands, and eccentric loading of the extensor muscles can build resilience. Instructors should introduce these exercises gradually, avoiding sharp pain. Over several weeks, improved muscular support can reduce the amount of force transmitted through the dorsal wrist structures during weight‑bearing poses.
5.3 Listening to Early Signals
The most useful habit is paying attention to the first signs of discomfort. A mild ache that resolves after practice may not be cause for concern, but pain that lingers into the next day or worsens with each class deserves attention. Instructors who modify their hand placement—using fists instead of flat palms, or shifting to forearm planks temporarily—can often prevent a minor irritation from becoming a chronic limitation.
FAQ
Q1: Is shockwave therapy painful for wrist overload conditions?
Most instructors describe a tapping or sharp sensation that is uncomfortable but brief. The wrist has less soft tissue coverage, so the feeling may be more pronounced, but the session length is short, and discomfort stops when the applicator lifts.
Q2: How many shockwave therapy sessions does a typical instructor need?
A common approach involves three to five sessions spaced one week apart. Some notice improvement after two sessions, while others benefit from a longer series. The full effect often appears several weeks after completing treatment.
Q3: Can I keep teaching yoga or Pilates during shockwave therapy?
Yes, most instructors continue teaching while receiving treatment. Avoiding the specific wrist positions that cause sharp pain may help. Using props such as wedges or blocks can reduce the wrist extension angle.
Q4: How soon after a shockwave session will I feel less wrist discomfort?
Some individuals notice a change within a few days. However, the most noticeable improvement typically occurs after several weeks as the tissue responds to the mechanical stimulus and remodeling takes place.
Q5: Does shockwave therapy work for carpal boss specifically?
Shockwave therapy does not remove the bony protuberance. However, it may reduce the surrounding soft tissue irritation and improve tendon gliding, which can lead to less discomfort during weight‑bearing activities.
Conclusion
Yoga and Pilates instructors devote their professional lives to helping others move with strength and ease. Yet the foundational postures of these practices—weight‑bearing through hyperextended wrists—can create persistent hand discomfort. Carpal bossing and wrist overload stem from repeated compression and friction between dorsal soft tissues and underlying bones. For instructors who have tried modifications without lasting relief, extracorporeal shockwave therapy offers a non‑invasive, drug‑free option. It works through mechanotransduction, improved blood flow, and modulation of pain signaling. When combined with sensible practice adjustments, gradual strengthening, and attention to early warning signs, shockwave therapy may help instructors maintain the wrist comfort they need to continue sharing the benefits of yoga and Pilates with their students.
References
American Society for Surgery of the Hand – Carpal Boss
https://www.assh.org/handcare/condition/carpal-boss
National Center for Biotechnology Information – Carpal Boss: A Review of Anatomy, Diagnosis, and Treatment
https://www.ncbi.nlm.nih.gov/books/NBK549902
Yoga Journal – Wrist Pain in Yoga: Causes and Modifications
https://www.yogajournal.com/practice/wrist-pain-in-yoga
Pilates Anytime – Protecting Your Wrists During Pilates Practice
https://www.pilatesanytime.com/blog/protecting-your-wrists
Extracorporeal Shockwave Therapy for Tendinopathies: A Systematic Review