
Introduction
For many recreational tennis players, the weekend represents a treasured escape from work and daily responsibilities—a time to step onto the court, enjoy friendly competition, and stay active. However, this pattern of compressing most physical activity into one or two days can place significant strain on the body. Among the most common overuse injuries affecting this population is Achilles tendinopathy, a degenerative condition of the large tendon at the back of the ankle. Research indicates that Achilles tendon problems occur in approximately 32% of tennis players seeking care for tendon-related issues. Recreational players between the ages of 35 and 45 appear particularly susceptible. This article explores what Achilles tendinopathy is, why weekend players face unique challenges, and how supportive approaches such as shockwave therapy may help manage symptoms and complement traditional rehabilitation.
1. Understanding Achilles Tendinopathy in Tennis
Before examining management options, it helps to understand what Achilles tendinopathy actually is and why tennis players develop this condition at higher rates than many other athletes.
1.1 What Is Achilles Tendinopathy?
Achilles tendinopathy refers to a degenerative condition of the Achilles tendon, not an inflammatory process. The term “tendinitis” is therefore not accurate for describing this chronic condition. The injury develops gradually from chronic repetitive movements during activities that involve running and jumping. Unlike an acute tendon tear that happens suddenly, tendinopathy results from accumulated microtrauma that exceeds the tendon‘s natural repair capacity. Over time, the collagen fibers within the tendon become disorganized, and degenerative changes occur within the tendon matrix. This condition typically causes pain localized to the tendon itself, often accompanied by morning stiffness that resolves after a few minutes of walking. It is both a persistent and potentially debilitating condition when left unaddressed.
1.2 How Common Is It Among Tennis Players?
Available data suggests that Achilles tendon problems are quite common among tennis players. In a study of athletes consulting a sports medicine unit, Achilles tendon injuries accounted for 14% of all sports-related visits, and tennis players represented 32% of those with Achilles issues—second only to joggers at 66%. This finding highlights the significant role that running and jumping movements play in the development of Achilles tendinopathy. Across different athletic populations, the prevalence of Achilles tendinopathy is approximately 6.2%, making it one of the most common lower limb tendinopathies alongside patellar tendinopathy. Among tennis players specifically, those aged 35 to 45 years appear to be the most frequently affected group.
1.3 Why Weekend Players Are at Greater Risk
The term “weekend warrior” describes individuals who engage in demanding recreational sporting activities on weekends despite minimal physical activity during the week. This pattern creates several problems for tendon health. First, the tendon does not receive gradual conditioning throughout the week, so it remains relatively deconditioned when Saturday arrives. Second, the sudden spike in activity volume—potentially several hours of tennis after five days of relative inactivity—places an abrupt increase in mechanical load on the Achilles tendon. Third, fatigue accumulates during these concentrated sessions, which may alter movement patterns and increase strain on the tendon. The combination of general deconditioning and excessive weekend activity predisposes these individuals to foot and ankle injuries, including Achilles tendinopathy.
2. Recognizing the Condition Early
Early recognition of Achilles tendinopathy allows players to adjust their activity before the condition progresses. The symptoms tend to develop gradually, and paying attention to early warning signs can make a meaningful difference.
2.1 Typical Symptoms
The symptoms of Achilles tendinopathy usually begin subtly. A player might notice pain in the back of the heel or lower calf at the start of a tennis session, which may improve temporarily as the tendon warms up. Morning stiffness around the tendon upon rising is another common feature, typically resolving after a few minutes of walking. As the condition progresses, the pain may become more persistent during activity and may even continue after play has stopped. Some players describe the discomfort as a dull ache, while others feel a more pronounced tenderness when pressing on the tendon. Swelling or nodular thickening of the tendon may also develop in later stages.
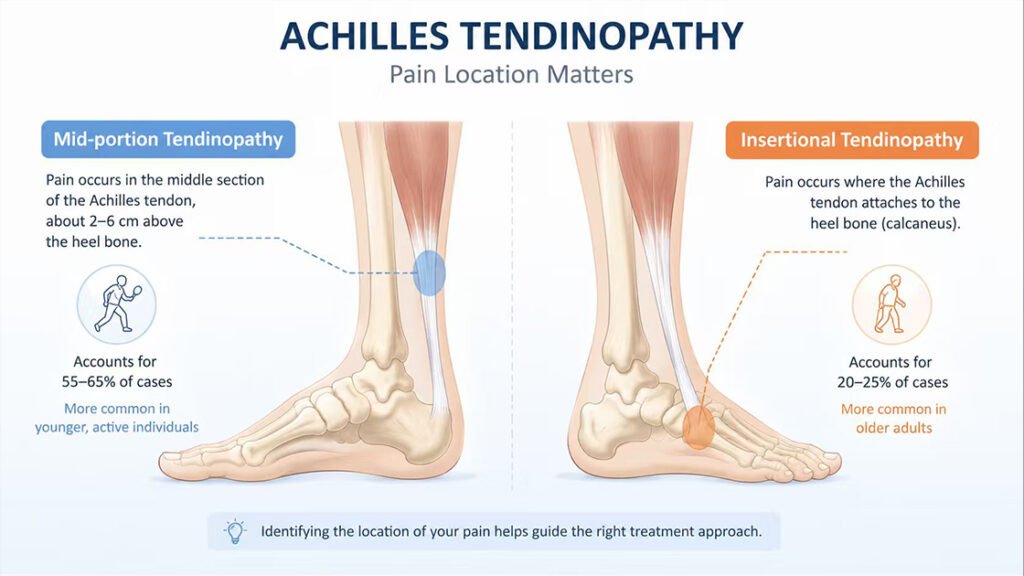
2.2 Pain Location Matters
The location of pain within the Achilles tendon provides useful information about the type of tendinopathy. Mid-portion tendinopathy involves pain approximately 2 to 6 centimeters above where the tendon inserts into the heel bone. This form accounts for about 55 to 65% of Achilles tendon injuries and is more common in younger, active individuals. Insertional tendinopathy affects the area where the tendon attaches to the calcaneus, representing approximately 20 to 25% of cases. This form is more common in older adults and may be associated with bony changes at the heel. Distinguishing between these two types matters for management decisions, as the approaches may differ slightly.
2.3 Why Ignoring Symptoms Can Be Problematic
Continuing to play through Achilles pain carries several risks. The degenerative changes within the tendon tend to worsen with continued overloading, potentially leading to more significant structural damage that requires longer recovery periods. The player may also unconsciously alter their movement patterns to avoid pain, which can place abnormal stress on other structures such as the plantar fascia, knee, or hip. Additionally, chronic Achilles tendinopathy that remains unmanaged may increase the risk of acute tendon rupture, a more serious injury that often requires immobilization or surgical intervention. Addressing symptoms early generally leads to shorter recovery times and fewer complications.
3. How Shockwave Therapy May Support Recovery
Shockwave therapy has emerged as a non-invasive option for managing chronic tendon conditions. Understanding how it works can help players make informed decisions about incorporating it into their recovery plan.
3.1 What Is Shockwave Therapy?
Extracorporeal shockwave therapy (ESWT) involves delivering high-energy acoustic pulses through the skin to the affected tendon tissue. Unlike radial pressure waves that dissipate at the skin‘s surface, focused shockwaves can penetrate deeper into the tendon structure. The therapy has been used for various tendinopathies, including plantar fasciitis, lateral epicondylitis (tennis elbow), patellar tendinopathy, and Achilles tendinopathy. It is considered a non-invasive intervention that aims to support the body’s natural healing processes. Treatment sessions typically last only a few minutes, and the procedure does not require any incisions or injections.
3.2 Potential Mechanisms of Action
Shockwave therapy may influence tendon healing through several physiological pathways. One proposed mechanism is mechanotransduction, where the acoustic pulses create controlled microtrauma within the tendon tissue. This microtrauma appears to trigger a biological healing response that stimulates tenocyte proliferation and collagen synthesis—essentially helping to restart the stalled repair process in chronic tendinopathy. Another potential mechanism involves neovascularization, where shockwave therapy promotes the expression of growth factors such as VEGF, leading to improved blood supply in tendon zones that normally have poor circulation. Additionally, shockwave therapy may influence pain signaling by reducing the concentration of substance P and affecting unmyelinated sensory nerve fibers, which may contribute to both short-term relief and longer-term functional improvement.
3.3 Evidence for Achilles Tendinopathy
Several systematic reviews and meta-analyses have examined the effectiveness of shockwave therapy for Achilles tendinopathy. A 2024 meta-analysis focusing on focused shockwave therapy found that when combined with a progressive loading program involving eccentric exercises, the approach resulted in higher return-to-sport rates compared to physiotherapy alone. For chronic Achilles tendinopathy specifically, focused shockwave has shown success in a significant percentage of patients who had not improved with standard conservative management. Another systematic review including 16 studies with 505 cases of Achilles tendinopathy found positive outcomes for both insertional and non-insertional types, with weighted mean post-treatment VAS pain scores decreasing from approximately 7 to 2.5 and VISA-A functional scores improving from approximately 45 to 75. These findings suggest that shockwave therapy may be a useful supportive tool for appropriate candidates.
3.4 What to Expect During Treatment
A typical shockwave therapy session involves applying a handheld device to the skin over the affected tendon. A coupling gel helps transmit the acoustic waves effectively. The practitioner moves the applicator across the treatment area, delivering pulses at a set frequency and energy level. Most patients describe the sensation as somewhat uncomfortable but tolerable, often comparing it to repeated tapping or snapping against the skin. A session usually lasts between 5 and 15 minutes, depending on the size of the area being treated. Multiple sessions may be recommended, often spaced several days or weeks apart. There is typically no downtime after treatment, meaning players can resume their normal daily activities immediately.
4. Integrating Shockwave With Conventional Approaches
Shockwave therapy works best as one component of a comprehensive management plan rather than as a standalone solution. Several other approaches play important roles in supporting tendon recovery.
4.1 The Role of Eccentric Loading
Eccentric exercise has been shown to be effective for the majority of cases of non-insertional Achilles tendinopathy. The key component involves the heel-drop eccentric portion of calf strengthening, where the player slowly lowers their heel below the level of a step while keeping the knee straight or slightly bent. This movement places a controlled stretch on the Achilles tendon while the calf muscle lengthens under tension. The exercise should be performed progressively, meaning the player gradually increases the number of repetitions and sets as tolerated. A small amount of discomfort during the exercise may be acceptable, but sharp or worsening pain suggests that the load needs to be reduced.
4.2 Activity Modification
Temporarily modifying tennis activities can help reduce mechanical loading on the Achilles tendon while allowing other forms of conditioning to continue. Reducing the frequency and duration of court time is usually the first step. Players may also consider switching to lower-impact activities such as swimming or cycling to maintain cardiovascular fitness without stressing the tendon. In the early stages of recovery, avoiding hill running, sprinting, and sudden directional changes can help prevent aggravation of symptoms. As the tendon settles, players can gradually reintroduce tennis-specific movements, starting with gentle groundstrokes before progressing to serves, volleys, and match play.
4.3 Appropriate Footwear and Orthotics
Proper footwear plays an important role in managing Achilles tendinopathy. Shoes with adequate cushioning and heel lift can reduce the strain on the tendon during walking and running. Some players benefit from using a small heel lift inside their everyday shoes, which effectively shortens the calf-Achilles complex and reduces tension on the tendon. For players with biomechanical factors such as forefoot varus or limited ankle dorsiflexion, custom orthotics may help address these underlying issues. A physical therapist or sports medicine professional can provide guidance on whether footwear modifications would be beneficial for a specific individual.
4.4 When Rest Is Appropriate
Complete rest is rarely necessary or desirable for Achilles tendinopathy. However, reducing activity to a level that does not provoke significant pain can help the tendon settle. The concept of relative rest means avoiding the specific movements that cause discomfort while maintaining other forms of exercise that do not stress the tendon. A good rule of thumb is that mild discomfort during activity may be acceptable as long as the pain subsides within a few hours after finishing and does not worsen from one session to the next. If pain persists or worsens, further activity reduction may be needed.
5. Practical Advice for Weekend Tennis Players
Balancing a love for tennis with the need for tendon recovery requires patience and a willingness to adjust routines. These practical considerations can help weekend players stay active while managing their symptoms.
5.1 Warming Up and Cooling Down
A proper warm-up before stepping onto the court prepares the Achilles tendon for the demands ahead. Gentle walking, light calf stretches, and ankle mobility exercises can increase blood flow and tissue elasticity. Players should avoid jumping straight into intense drills or match play without a gradual warm-up period. After playing, a cool-down that includes light stretching and perhaps gentle self-massage of the calf muscles can help reduce post-activity stiffness. Some players find that applying a cold pack to the tendon for 10 to 15 minutes after tennis helps manage any lingering discomfort, although this should not be seen as a substitute for other management strategies.
5.2 Listening to Pain Signals
Pain serves as an important signal from the body about tissue tolerance. For Achilles tendinopathy, the mantra “let pain be your guide” generally applies. A small amount of discomfort during eccentric exercises or modified tennis may be acceptable as long as it does not significantly worsen during or after activity. However, sharp or increasing pain that persists after rest suggests that the loading needs to be reduced. Keeping a simple daily log of pain levels and activity can help players track their progress and identify patterns. If pain consistently worsens over several weeks despite appropriate management, consulting a healthcare provider is recommended.
5.3 Setting Realistic Return-to-Play Expectations
Returning to full tennis activity takes time. Most players with Achilles tendinopathy can expect a recovery period of several weeks to a few months, depending on the severity and duration of symptoms before treatment. A phased return that progresses from low-impact conditioning to tennis-specific movements to full match play tends to work well. Players should resist the urge to rush back simply because a tournament or social match is approaching. Returning too quickly often leads to setbacks that prolong the overall recovery time. Patience and consistency with rehabilitation exercises typically produce better long-term outcomes than aggressive early return to play.
5.4 Knowing When to Seek Professional Guidance
While mild cases of Achilles tendinopathy may improve with activity modification and eccentric exercises, certain situations warrant professional evaluation. If pain persists for more than several weeks despite appropriate self-management, or if the player notices a visible nodule or thickening of the tendon, consulting a healthcare provider is advisable. Physical therapists and sports medicine physicians can perform a thorough assessment, confirm the diagnosis, and design a tailored rehabilitation program. They can also determine whether additional interventions such as shockwave therapy would be appropriate for the individual‘s specific presentation.
Frequently Asked Questions
Q1: Can I still play tennis with Achilles tendinopathy?
You may continue with reduced frequency and intensity, but playing through significant pain usually worsens the condition. Activity modification helps.
Q2: How long does recovery typically take?
Recovery varies depending on severity and duration of symptoms. Most players improve over several weeks to a few months with appropriate management.
Q3: Is shockwave therapy painful?
Most patients describe the sensation as uncomfortable but tolerable. The procedure does not require anesthesia and has no downtime afterward.
Q4: Does shockwave therapy work for all types of Achilles tendinopathy?
Research suggests positive outcomes for both insertional and non-insertional tendinopathy. A healthcare provider can determine whether it suits your specific case.
Q5: How many shockwave sessions are typically needed?
The number varies, but many protocols involve three to five sessions spaced several days or weeks apart. Your practitioner will recommend a schedule based on your response.
Q6: Will shockwave therapy allow me to return to tennis faster?
The therapy may support symptom management and complement rehabilitation, but returning to full activity still requires patience and appropriate loading progression.
Conclusion
Achilles tendinopathy presents a genuine challenge for recreational tennis players who compress most of their physical activity into weekend sessions. Understanding the degenerative nature of this condition, recognizing early warning signs, and respecting the body‘s need for appropriate loading and recovery can help players stay active while managing their symptoms. Shockwave therapy offers a non-invasive supportive tool that may help stimulate the body’s natural healing processes when used alongside eccentric exercises, activity modification, and appropriate footwear. However, it is important to remember that shockwave therapy does not directly heal the tendon on its own—it works as part of a broader plan that includes gradual return to activity. With patience, consistency, and appropriate professional guidance, most weekend tennis players can look forward to returning to the court when their tendons are ready.
References
Kvist, M. (1991). Achilles tendon injuries in athletes.
https://pubmed.ncbi.nlm.nih.gov/1897886
ITF Tennis. Achilles Tendon Injury Fact Sheet.
https://www.itftennis.com/media/2132/injury-achilles-tendon.pdf
Kvist, M. Achilles tendon injuries in athletes. Ann Chir Gynaecol. 1991.
https://read.qxmd.com/read/1897886/achilles-tendon-injuries-in-athletes
Bowen, C., et al. (2024). The ‘weekend warrior’: Fact or fiction for major trauma? Canadian Journal of Surgery.
https://pmc.ncbi.nlm.nih.gov/articles/PMC4266932
Head2Toe Osteopathy. (2026). From Road to Recovery: Focused Shockwave Therapy for Runner‘s Tendinopathy.
Stania, M., Malá, J., & Chmielewska, D. (2024). The Efficacy of Extracorporeal Shock Wave Therapy as a Monotherapy for Achilles Tendinopathy: A Systematic Review and Meta-Analysis.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11141754
Wu, J., et al. (2022). A Systematic Review of Extracorporeal Shock Wave Therapy (ESWT) for Insertional and Non-Insertional Achilles Tendinopathy.
https://pmc.ncbi.nlm.nih.gov/articles/PMC9703551
ShockwaveMachines.com. How Shockwave Therapy Works.
https://www.shockwavemachines.com/how-shockwave-therapy-works
ShockwaveMachines.com. Shockwave Therapy Protocols.
https://www.shockwavemachines.com/shockwave-therapy-protocols